In this Belgian study, 112 participants with varying cognitive decline degrees were included. Radiologists manually assessed medial temporal lobe atrophy (MTA), a common indicator of Alzheimer's, achieving a sensitivity of 0.778 and specificity of 0.938. This was compared to icobrain dm, which involved calculating the ILV (inferior lateral ventricle) to hippocampal volume ratio, resulting in a sensitivity of 0.96 and specificity of 0.88, effectively differentiating Alzheimer's patients from cognitively normal individuals. The authors suggest that the ILV/Hip ratio score can serve as an additional metric for MTA atrophy stage and progression.
Read full study.
Abstract
Purpose
To assess the performance of the inferior lateral ventricle (ILV) to hippocampal (Hip) volume ratio on brain MRI, for Alzheimer’s disease (AD) diagnostics, comparing it to individual automated ILV and hippocampal volumes, and visual medial temporal lobe atrophy (MTA) consensus ratings.
Methods
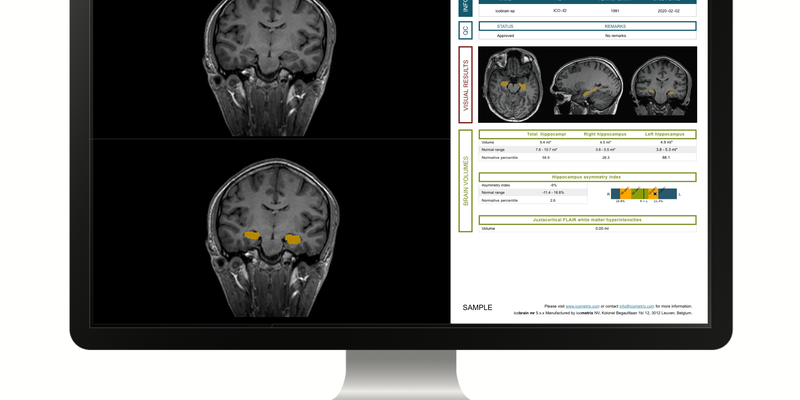
One-hundred-twelve subjects (mean age ± SD, 66.85 ± 13.64 years) with varying degrees of cognitive decline underwent MRI using a Philips Ingenia 3T. The MTA scale by Scheltens, rated on coronal 3D T1-weighted images, was determined by three experienced radiologists, blinded to diagnosis and sex. Automated volumetry was computed by icobrain dm (v. 5.10) for total, left, right hippocampal, and ILV volumes. The ILV/Hip ratio, defined as the percentage ratio between ILV and hippocampal volumes, was calculated and compared against a normative reference population (n = 1903). Inter-rater agreement, association, classification accuracy, and clinical interpretability on patient level were reported.
Results
Visual MTA scores showed excellent inter-rater agreement. Ordinal logistic regression and correlation analyses demonstrated robust associations between automated brain segmentations and visual MTA ratings, with the ILV/Hip ratio consistently outperforming individual hippocampal and ILV volumes. Pairwise classification accuracy showed good performance without statistically significant differences between the ILV/Hip ratio and visual MTA across disease stages, indicating potential interchangeability. Comparison to the normative population and clinical interpretability assessments showed commensurability in classifying MTA “severity” between visual MTA and ILV/Hip ratio measurements.
Conclusion
The ILV/Hip ratio shows the highest correlation to visual MTA, in comparison to automated individual ILV and hippocampal volumes, offering standardized measures for diagnostic support in different stages of cognitive decline.