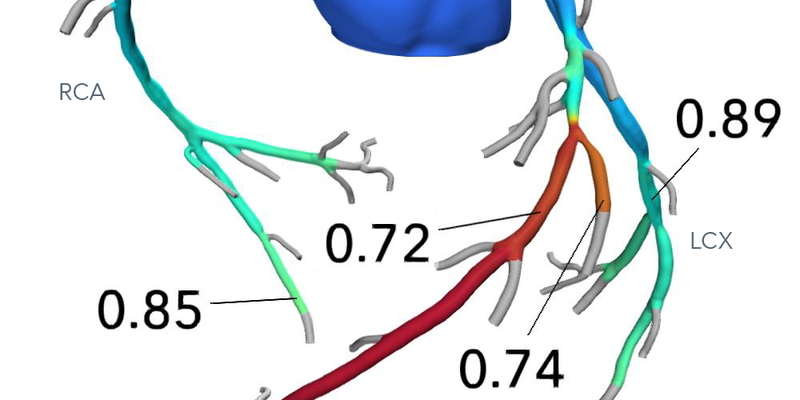
A multinational study evaluated HeartFlow's CT angiography-derived fractional flow reserve (FFRCT) analysis tool on 102 patients (156 vessels) with stable coronary artery disease, comparing its predictions with invasive FFR outcomes, focusing on identifying target vessel failure (TVF) risks. Including 20 vessels with TVF over a median follow-up of 9.9 years, the study revealed that FFRCT ≤0.80 had a hazard ratio of 2.61, validating its predictive accuracy for clinical outcomes similar to invasive FFR (c-index 0.79 vs. 0.71). In 94 vessels where percutaneous coronary intervention (PCI) was deferred, there was an inverse relationship between FFRCT and TVF risk (HR 0.62 per 0.1 FFRCT increase), with cumulative incidences of 2.6%, 15.2%, and 28.6% for FFRCT >0.90, 0.81–0.90, and ≤0.80 respectively. These findings emphasize the AI tool's potential in enhancing treatment decisions and guidelines by evaluating future coronary event risks upon intervention deferral.
Read full study.
Abstract
Background & Objectives
The long-term prognostic implications of CT angiography-derived fractional flow reserve (FFRCT) remains unclear. We aimed to explore the long-term outcomes of FFRCT in the first-in-human study of it.
Materials & methods
A total of 156 vessels from 102 patients with stable coronary artery disease, who underwent coronary CT angiography (CCTA) and invasive FFR measurement, were followed. The primary endpoint was target vessel failure (TVF), including cardiovascular death, target vessel myocardial infarction, and target vessel revascularization. Outcome analysis with FFRCT was performed on a per-vessel basis using a marginal Cox proportional hazard model.
Results
During median 9.9 years of follow-up, TVF occurred in 20 (12.8%) vessels. FFRCT ≤0.80 discriminated TVF (hazard ratio [HR] 2.61, 95% confidence interval [CI] 1.06, 6.45). Among 94 vessels with deferral of percutaneous coronary intervention (PCI), TVF risk was inversely correlated with FFRCT (HR 0.62 per 0.1 increase, 95% CI 0.44, 0.86), with the cumulative incidence of TVF being 2.6%, 15.2%, and 28.6% for vessels with FFRCT >0.90, 0.81–0.90, and ≤0.80, respectively (p-for-trend 0.005). Predictive value for clinical outcomes of FFRCT was similar to that of invasive FFR (c-index 0.79 vs 0.71, P = 0.28). The estimated TVF risk was higher in the deferral of PCI group than the PCI group for vessels with FFRCT ≤0.81.
Conclusion
FFRCT showed improved long-term risk stratification and displayed a risk continuum similar to invasive FFR.