A Japanese prospective study evaluated Us2.v1 (Us2.ai), an AI tool for echocardiographic analysis, using echocardiograms of 23 participants with various cardiac conditions including ischemic heart disease, arrhythmia, hypertrophic cardiomyopathy, severe pulmonary hypertension, and severe aortic stenosis. The study aimed to compare the time efficiency and diagnostic accuracy of echocardiographic examinations performed by a human expert versus those analyzed by the fully automated US2.ai software. The assistance of the US2.ai tool led to a significant reduction in measurement time (159 ± 66 s vs. 325 ± 94 s, p < 0.01) and report creation time (71 ± 39 s vs. 429 ± 128 s, p < 0.01), demonstrating the software's capacity to provide rapid and automated parameter assessment. This resulted in an overall 70% reduction in the time required for measurement and report creation compared to manual methods, while maintaining high accuracy for most echocardiographic parameters. However, for fair or poor image quality, AI needed more corrections, extending measurement and report creation times, especially in complex reports requiring human confirmation of AI findings.
Read full study.
Abstract
Background
Manual interpretation of echocardiographic data is time-consuming and operator-dependent. With the advent of artificial intelligence (AI), there is a growing interest in its potential to streamline echocardiographic interpretation and reduce variability. This study aimed to compare the time taken for measurements by AI to that by human experts after converting the acquired dynamic images into DICOM data.
Methods
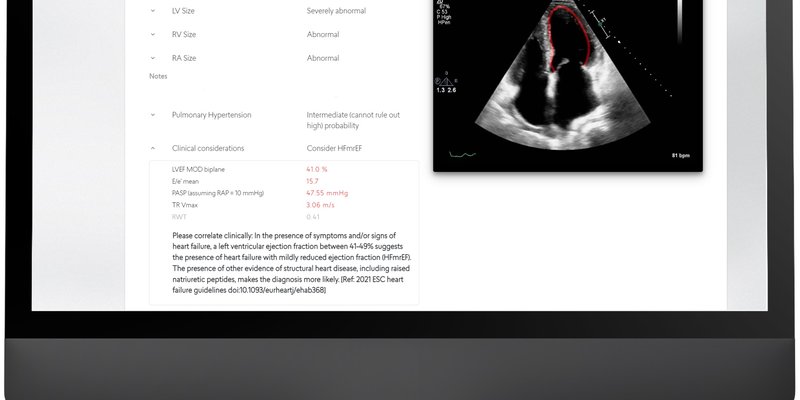
Twenty-three consecutive patients were examined by a single operator, with varying image quality and different medical conditions. Echocardiographic parameters were independently evaluated by human expert using the manual method and the fully automated US2.ai software. The automated processes facilitated by the US2.ai software encompass real-time processing of 2D and Doppler data, measurement of clinically important variables (such as LV function and geometry), automated parameter assessment, and report generation with findings and comments aligned with guidelines. We assessed the duration required for echocardiographic measurements and report creation.
Results
The AI significantly reduced the measurement time compared to the manual method (159 ± 66 vs. 325 ± 94 s, p < 0.01). In the report creation step, AI was also significantly faster compared to the manual method (71 ± 39 vs. 429 ± 128 s, p < 0.01). The incorporation of AI into echocardiographic analysis led to a 70% reduction in measurement and report creation time compared to manual methods. In cases with fair or poor image quality, AI required more corrections and extended measurement time than in cases of good image quality. Report creation time was longer in cases with increased report complexity due to human confirmation of AI-generated findings.
Conclusions
This fully automated software has the potential to serve as an efficient tool for echocardiographic analysis, offering results that enhance clinical workflow by providing rapid, zero-click reports, thereby adding significant value.