A German retrospective study evaluated CorEx by Spimed-AI, an AI tool for photon-counting coronary computed tomography angiography (PC-CCTA) stenosis detection and artificial intelligence-derived fractional flow reserve (FFRai), using CT scans of 260 participants with severe symptomatic aortic valve stenosis undergoing work-up for transcatheter aortic valve replacement (TAVR), with invasive coronary angiography (ICA) as the reference standard. Out of the participants, 126/260 had significant coronary artery disease. The CorEx tool achieved a per-patient sensitivity of 96.0% for PC-CCTA and 96.8% for FFRai, along with specificities of 68.7% and 87.3%, respectively. Its application could have avoided the need for diagnostic ICA in 121 out of 260 patients (46.5%), highlighting its potential to significantly reduce invasive diagnostic procedures in the clinical TAVR work-up.
Read full study
Abstract
Purpose
The purpose of this study was to evaluate the capabilities of photon-counting (PC) CT combined with artificial intelligence-derived coronary computed tomography angiography (PC-CCTA) stenosis quantification and fractional flow reserve prediction (FFRai) for the assessment of coronary artery disease (CAD) in transcatheter aortic valve replacement (TAVR) work-up.
Materials and methods
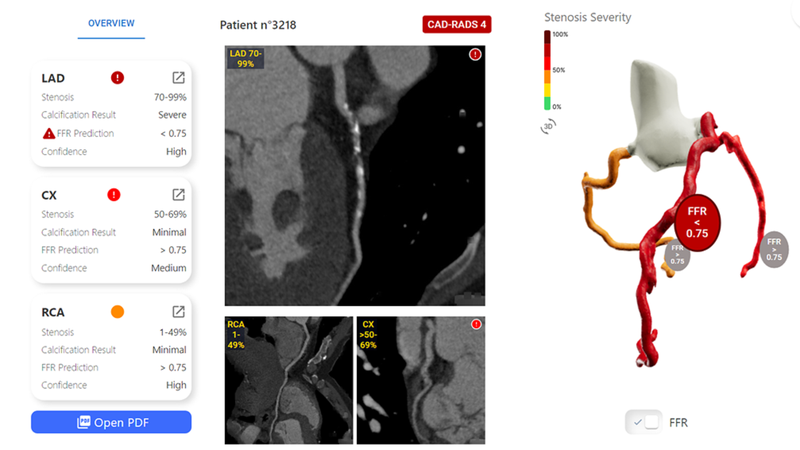
Consecutive patients with severe symptomatic aortic valve stenosis referred for pre-TAVR work-up between October 2021 and June 2023 were included in this retrospective tertiary single-center study. All patients underwent both PC-CCTA and ICA within three months for reference standard diagnosis. PC-CCTA stenosis quantification (at 50% level) and FFRai (at 0.8 level) were predicted using two deep learning models (CorEx, Spimed-AI). Diagnostic performance for global CAD evaluation (at least one significant stenosis ≥ 50% or FFRai ≤ 0.8) was assessed.
Results
A total of 260 patients (138 men, 122 women) with a mean age of 78.7 ± 8.1 (standard deviation) years (age range: 51–93 years) were evaluated. Significant CAD on ICA was present in 126/260 patients (48.5%). Per-patient sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy were 96.0% (95% confidence interval [CI]: 91.0–98.7), 68.7% (95% CI: 60.1–76.4), 74.3 % (95% CI: 69.1–78.8), 94.8% (95% CI: 88.5–97.8), and 81.9% (95% CI: 76.7–86.4) for PC-CCTA, and 96.8% (95% CI: 92.1–99.1), 87.3% (95% CI: 80.5–92.4), 87.8% (95% CI: 82.2–91.8), 96.7% (95% CI: 91.7–98.7), and 91.9% (95% CI: 87.9–94.9) for FFRai. Area under the curve of FFRai was 0.92 (95% CI: 0.88–0.95) compared to 0.82 for PC-CCTA (95% CI: 0.77–0.87) (P < 0.001). FFRai-guidance could have prevented the need for ICA in 121 out of 260 patients (46.5%) vs. 97 out of 260 (37.3%) using PC-CCTA alone (P < 0.001).
Conclusion
Deep learning-based photon-counting FFRai evaluation improves the accuracy of PC-CCTA ≥ 50% stenosis detection, reduces the need for ICA, and may be incorporated into the clinical TAVR work-up for the assessment of CAD.
