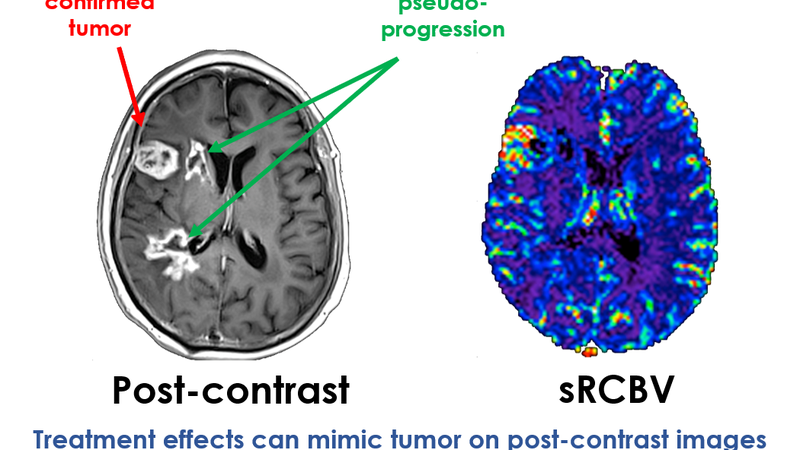
A U.S. retrospective study evaluated IB Neuro (Imaging Biometrics), an AI tool designed to enhance diagnostic precision in the post-treatment surveillance of High-Grade Gliomas (HGGs), using MRI scans of 45 participants. IB Neuro integrated Dynamic Susceptibility Contrast Relative Cerebral Blood Volume (DSC-rCBV) and Dynamic Susceptibility Contrast Fractional Tumor Burden (DSC-FTB) into standard contrast-enhanced MRI (CE-MRI) to better identify tumor recurrence versus post-treatment effects. This integration led to improved consensus among four radiologists with varying experience, with interrater agreement growing from standard contrast-enhanced MRI alone (κ = 0.63) to DSC-rCBV (κ = 0.66) and achieving the highest with DSC-FTB (κ = 0.70). The highest agreement between raters and a consensus was with DSC-FTB (κ = 0.66–0.80). Clinically meaningful changes in MR imaging interpretations were seen in up to 20% of patients by adding these perfusion metrics, marking a potential impact on clinical management adjustments.
Read full study
Arterial Spin-Labeling and DSC Perfusion Metrics Improve Agreement in Neuroradiologists’ Clinical Interpretations of Posttreatment High-Grade Glioma Surveillance MR Imaging—An Institutional Experience
American Journal of Neuroradiology, 2024
Abstract
Background and purpose: MR perfusion has shown value in the evaluation of posttreatment high-grade gliomas, but few studies have shown its impact on the consistency and confidence of neuroradiologists’ interpretation in routine clinical practice. We evaluated the impact of adding MR perfusion metrics to conventional contrast-enhanced MR imaging in posttreatment high-grade glioma surveillance imaging.
Materials and Methods: This retrospective study included 45 adults with high-grade gliomas who had posttreatment perfusion MR imaging. Four neuroradiologists assigned Brain Tumor Reporting and Data System scores for each examination on the basis of the interpretation of contrast-enhanced MR imaging and then after the addition of arterial spin-labeling-CBF, DSC-relative CBV, and DSC-fractional tumor burden. Interrater agreement and rater agreement with a multidisciplinary consensus group were assessed with κ statistics. Raters used a 5-point Likert scale to report confidence scores. The frequency of clinically meaningful score changes resulting from the addition of each perfusion metric was determined.
Results: Interrater agreement was moderate for contrast-enhanced MR imaging alone (κ = 0.63) and higher with perfusion metrics (arterial spin-labeling-CBF, κ = 0.67; DSC-relative CBV, κ = 0.66; DSC-fractional tumor burden, κ = 0.70). Agreement between raters and consensus was highest with DSC-fractional tumor burden (κ = 0.66–0.80). Confidence scores were highest with DSC-fractional tumor burden. Across all raters, the addition of perfusion resulted in clinically meaningful interpretation changes in 2%–20% of patients compared with contrast-enhanced MR imaging alone.
Conclusions: Adding perfusion to contrast-enhanced MR imaging improved interrater agreement, rater agreement with consensus, and rater confidence in the interpretation of posttreatment high-grade glioma MR imaging, with the highest agreement and confidence scores seen with DSC-fractional tumor burden. Perfusion MR imaging also resulted in interpretation changes that could change therapeutic management in up to 20% of patients.
