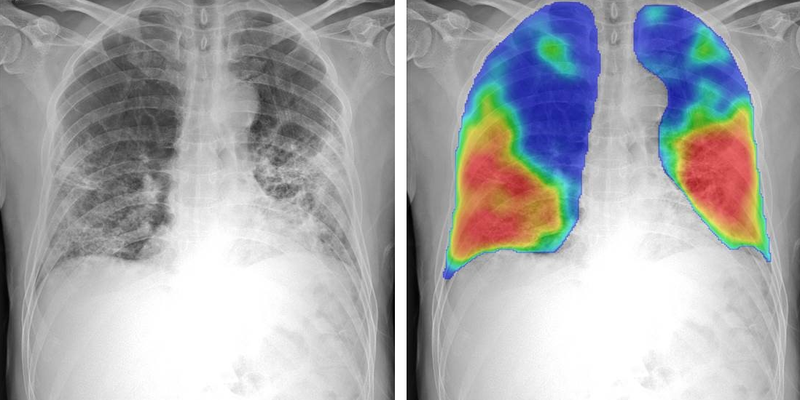
Company: Delft Imaging Product: CAD4TB
Clinical evaluation of computer-aided digital x-ray detection of pulmonary tuberculosis during community-based screening or active case-finding: a case-control study
The Lancet Global Health, 2025
Abstract
Background
Computer-aided detection (CAD) has been recommended as a tuberculosis screening tool. However, there are limited data about its utility, specifically in a community-based setting where the targeted population and the highest burden of undetected individuals resides. The aim of this study was to evaluate the diagnostic accuracy and clinical utility of CAD during community-based active case-finding (ACF) for tuberculosis.
Methods
In this case-control study, we used individual patient data from adults aged 15 years or older who resided in tuberculosis-endemic or HIV-endemic communities, pooled from five community-based ACF studies in South Africa from November, 2016 to August, 2023. Cases were defined as participants who were tuberculosis positive (diagnosed with pulmonary tuberculosis by sputum Xpert Ultra or culture positivity, or both) and controls were tuberculosis negative. Controls were randomly sampled from each study at an approximate 1:2 ratio (case to control). We assessed CAD-interpreted chest radiography (CAD4TB version 7) against a microbiological reference standard. Diagnostic accuracy of CAD was determined by sensitivity, specificity, and area under the receiver operating curve (AUC). CAD performance was additionally assessed in various subgroups. We evaluated the clinical utility of CAD and performed a preliminary cost analysis comparing the cost per tuberculosis case detected and initiated on treatment (per 10 000 individuals screened) for two community-based diagnostic strategies: Xpert Ultra in everyone screened versus Xpert Ultra only in CAD-positive individuals.
Findings
Of the 20 770 individuals enrolled across all studies, 530 (2·6%) had microbiologically proven tuberculosis. Data were available for 501 (94·5%) of the individuals with tuberculosis (cases) and 938 tuberculosis-negative individuals (controls). CAD achieved an AUC of 0·83 (95% CI 0·80-0·85). At a fixed sensitivity of 90% (threshold: 5) specificity was 44·9% (95% CI 42·5-47·3) and at a fixed sensitivity of 85% (threshold: 10) specificity was 54·1% (51·7-56·5). In the subgroup analysis, CAD performed worse in people living with HIV compared with HIV-negative people (AUC of 0·76 [0·71-0·81] vs 0·85 [0·82-0·87]; p=0·0037) and in asymptomatic people compared with symptomatic people (0·79 [0·76-0·82] vs 0·85 [0·82-0·88]; p=0·0079. Nevertheless, a CAD-directed Xpert Ultra strategy reduced costs by 20-53% compared with a universal Xpert Ultra only strategy (US$2207-$3745 vs $4698 per tuberculosis case detected and initiated on treatment per 10 000 people screened), at the detriment of lower diagnostic yield (40-59% vs 65% per 10 000 individuals screened).
Interpretation
In the setting of community-based ACF, CAD did not meet the WHO screening test target product profile (>90% sensitivity and >70% specificity) and performed more poorly in some subgroups. However, a context-specific CAD-directed strategy could still be cost saving. These data inform community-based ACF strategies aiming to disrupt the tuberculosis transmission cycle.
Read full study